
PDA Autism: Understanding Demand Avoidance and Supporting Your Child
A child who repeatedly refuses everyday requests may be described as stubborn, controlling, oppositional or badly behaved.
For some autistic children, however, avoiding demands is not a deliberate attempt to challenge adults. It can be an intense response to anxiety, uncertainty, pressure or a perceived loss of control.
This pattern is commonly described as Pathological Demand Avoidance, or PDA. Many autistic people and families prefer the term Persistent Drive for Autonomy, as it focuses on the person’s powerful need to retain control over their actions and environment.
PDA is not currently recognised as a separate diagnosis. It is generally understood as a profile that may be present in some autistic people.
Recognising the reasons behind demand avoidance can transform the support a child receives. Instead of asking:
“How do we make this child comply?”
It may be more helpful to ask:
“What is making this demand feel unsafe, overwhelming or impossible?”
Parents who are beginning to explore their child’s wider presentation may also find our autism support for parents helpful.
What does PDA mean?
It describes a pattern in which a person experiences an unusually strong need to avoid everyday demands, expectations and perceived pressure.
The word “pathological” is controversial. Some autistic people feel it presents them as disordered, difficult or deliberately non-compliant. For this reason, terms such as Persistent Drive for Autonomy and Pervasive Drive for Autonomy are increasingly used.
Whatever terminology is preferred, PDA involves more than occasionally refusing instructions.
Most children avoid demands at times, especially when they are tired, anxious, distracted or uninterested. A PDA profile is more likely to involve avoidance that is:
- persistent and pronounced;
- present across different parts of everyday life;
- connected to a strong need for autonomy or control;
- triggered by demands that may appear small or reasonable;
- capable of affecting enjoyable activities as well as unwanted ones;
- associated with escalating anxiety, distress or dysregulation.
Demand avoidance should therefore be considered within the child’s wider pattern of development, communication, sensory processing, emotional regulation and daily functioning.
Is PDA a type of autism?
PDA is usually discussed as a profile within the autism spectrum, rather than as a separate type of autism or an independent medical diagnosis.
It does not currently appear as a standalone diagnosis in the principal diagnostic classifications used by clinicians. There is also no single assessment tool that can independently confirm PDA.
In practice, an assessment report may use wording such as:
- autism with a PDA profile;
- autism with marked demand avoidance;
- autism with an extreme demand-avoidant presentation;
- autism with a strong need for autonomy and control;
- autism accompanied by significant anxiety around demands.
Other clinicians may describe the child’s individual characteristics and support needs without using the term PDA.
This inconsistency can be frustrating for parents. However, the absence of a formal PDA diagnosis does not mean that the child’s needs should be dismissed.
Educational and therapeutic support should be based on the child’s identified difficulties and functional needs, rather than depending entirely on whether a particular label has been recorded.
Families considering professional assessment can read more about ADHD and ASD assessments and what an assessment can contribute to understanding a child’s needs.
Why do children with a PDA profile avoid demands?
There is unlikely to be one simple cause.
Demand avoidance may arise from a combination of:
- anxiety;
- intolerance of uncertainty;
- sensory overload;
- communication difficulties;
- fear of failure;
- executive-function difficulties;
- difficulty beginning or changing activities;
- previous distressing experiences;
- reduced trust in adults or environments;
- a strong need to preserve autonomy;
- difficulty predicting what will happen next.
For some children, a demand appears to trigger an immediate threat response.
The child may understand intellectually that brushing their teeth, getting dressed or entering a classroom is safe. Their nervous system may nevertheless react as though control is being removed and danger is approaching.
This can activate survival responses such as:
- Fight: shouting, arguing, hitting, pushing or threatening.
- Flight: running away, hiding or attempting to leave.
- Freeze: becoming unable to speak, move or begin the task.
- Fawn: agreeing, pleasing, joking or masking to escape immediate pressure.
- Shutdown: becoming withdrawn, exhausted or unresponsive.
This helps explain why repeating instructions, introducing sanctions or escalating consequences may increase distress rather than improve cooperation.
The behaviour may look deliberate from the outside, but the child’s ability to respond can reduce sharply when they feel threatened or controlled.
What counts as a demand?
A demand does not have to be a direct instruction such as “Put your shoes on.”
A child may experience pressure from several different sources.
Direct demands
Direct demands include clear requests or instructions such as:
- get dressed;
- complete your homework;
- sit at the table;
- stop playing;
- answer the question;
- go into the classroom;
- turn off the computer.
Even polite instructions may still feel demanding if the child believes that refusal is not genuinely permitted.
Indirect demands
A child may detect an expectation even when nobody has stated it directly.
Examples include:
- seeing a school uniform laid out;
- noticing that everyone is preparing to leave;
- being handed a worksheet;
- seeing a visual timetable;
- hearing that a visitor is arriving;
- noticing that dinner has been placed on the table.
The child may react to the implied expectation rather than the words being used.
Internal demands
Physical and emotional needs can also become demands.
These may include:
- hunger;
- thirst;
- tiredness;
- needing the toilet;
- feeling too hot or cold;
- noticing pain;
- recognising that they need help.
A child may delay eating, drinking, sleeping or using the toilet because responding to the bodily signal itself feels like surrendering control.
Self-imposed demands
A child can become unable to complete something they genuinely want to do once it begins to feel expected.
Examples include:
- opening a birthday present while people watch;
- attending a party they wanted to attend;
- finishing a favourite project;
- playing a game after agreeing to play;
- going on a planned family trip;
- beginning an activity they suggested themselves.
This apparent contradiction can be confusing for adults. The difficulty may not be the activity itself. It may be the pressure, expectation or loss of control that has become attached to it.
Demands created by praise
Even positive attention may create pressure.
Statements such as “You did that brilliantly yesterday” or “I know you can do it” may communicate an expectation that the child must repeat the same performance.
Some children therefore find public praise uncomfortable. Quiet acknowledgement, neutral feedback or allowing the child to recognise their own achievement may be better tolerated.
Demands created by rewards
Reward charts and incentive systems can turn an ordinary activity into a visible test of compliance.
For some children, this increases pressure rather than motivation. The child may now feel that they are being observed, evaluated or controlled.
Rewards are not automatically inappropriate, but they should not replace efforts to understand why the child is struggling.
Common signs of a PDA profile
No single behaviour proves that a child has a PDA profile.
Professionals should consider the wider pattern, the reasons behind the behaviour, the settings in which it occurs and the effect it has on daily life.
Possible characteristics include the following.
1. Avoiding ordinary everyday activities
The child may experience significant difficulty with routine activities such as:
- washing;
- dressing;
- eating;
- leaving home;
- entering school;
- completing work;
- attending appointments;
- going to bed.
The level of distress may appear out of proportion to the demand itself.
2. Using socially sophisticated avoidance strategies
Avoidance may involve:
- changing the subject;
- making jokes;
- distracting the adult;
- negotiating;
- delaying;
- offering elaborate explanations;
- pretending not to hear;
- creating a game;
- saying they feel unwell;
- giving reasons why the task cannot be completed.
These strategies can be mistaken for manipulation.
It is often more accurate to view them as attempts to escape pressure before the child becomes overwhelmed.
3. Appearing socially confident while struggling underneath
Some children with a PDA profile appear sociable, imaginative and verbally confident.
They may nevertheless experience difficulty:
- understanding social boundaries;
- tolerating other people’s expectations;
- managing relationships;
- accepting that somebody else is in control;
- recognising the effect of their behaviour;
- regulating themselves during social interaction.
Social fluency should not automatically be interpreted as social ease.
4. A strong need to control situations
The child may feel compelled to decide:
- what happens;
- when it happens;
- who participates;
- where people sit;
- which words adults use;
- how a task is completed;
- how a game or conversation develops.
This can look domineering. However, control may provide the predictability and safety the child is struggling to create internally.
5. Rapid emotional changes
A child may move quickly from calm and playful to frightened, angry, distressed or shut down.
The apparent trigger may be small, but stress may have accumulated throughout the day.
The final request is not always the true cause of the reaction.
6. Becoming absorbed in fantasy or role play
Imagination can be a strength and a means of emotional regulation.
Some children use characters, stories or role play to create distance from a demand. A request directed to a character may feel safer than a request directed personally to the child.
Role play should not automatically be treated as avoidance that must be stopped. It may provide a bridge into communication, learning or cooperation.
7. Avoiding enjoyable activities
Demand avoidance can affect:
- hobbies;
- celebrations;
- family outings;
- clubs;
- friendships;
- preferred lessons;
- special interests.
The child may desperately want to participate while also feeling unable to do so once attendance becomes expected.
8. Difficulty accepting praise
Praise may create:
- attention;
- embarrassment;
- expectation;
- fear of failure;
- pressure to repeat the achievement.
Low-key, specific and private recognition may therefore be more helpful than enthusiastic public praise.
9. Masking at school
Some children suppress their distress in structured settings and appear polite, cooperative, quiet or academically capable.
After school, they may experience:
- meltdowns;
- crying;
- anger;
- aggression;
- withdrawal;
- sleep difficulties;
- physical exhaustion;
- refusal to attend the following day.
The child may have used all their available energy to meet expectations during the school day.
A child who appears to cope in school may therefore still have substantial unmet needs. This is particularly important when gathering evidence for an EHCP, because parent observations can help demonstrate what happens outside the classroom.
10. Escalating when pressure increases
When adults repeat instructions, insist on immediate compliance or introduce consequences, the child may become less able to respond.
This does not mean all expectations must be removed. It means adults should consider whether their approach is inadvertently increasing the child’s sense of threat.
PDA, ordinary avoidance and autistic demand avoidance
Demand avoidance is not exclusive to PDA.
A child may avoid a request because they:
- do not understand it;
- cannot process the language quickly enough;
- are distracted;
- are exhausted;
- are experiencing sensory discomfort;
- fear making a mistake;
- cannot plan the steps involved;
- do not understand the purpose;
- are anxious about what will happen next;
- have experienced distress in the same situation previously.
Many autistic children experience some degree of demand avoidance without fitting a PDA profile.
PDA is generally used to describe a broader and more persistent pattern involving marked demand avoidance, a strong need for autonomy and the use of multiple strategies to escape expectations.
The distinction should not become more important than understanding the individual child.
Whether or not professionals use the PDA label, the child still requires support that addresses the reasons behind their distress.
For a wider explanation of how autism, ADHD and additional needs can affect education, see our practical SEN support, neurodiversity, ADHD and autism guide.
PDA and oppositional behaviour
PDA can sometimes be confused with oppositional behaviour or Oppositional Defiant Disorder, commonly abbreviated to ODD.
Both presentations can involve:
- refusal;
- arguing;
- anger;
- conflict with adults;
- apparent rule-breaking;
- attempts to control situations.
The underlying reasons may be different.
In a PDA presentation, resistance is often connected to anxiety, perceived threat, uncertainty and loss of autonomy.
A professional assessment should look beyond what the behaviour resembles and consider:
- what happens before it;
- what the child appears to fear or avoid;
- the role of sensory and communication needs;
- whether the behaviour changes when pressure is reduced;
- differences between home and school;
- the child’s developmental history;
- possible autism, ADHD, anxiety, trauma or learning needs.
Labels based solely on outward behaviour can result in the wrong interventions being used.
PDA and ADHD
PDA and ADHD can overlap.
A child with ADHD may struggle to respond to instructions because of:
- distractibility;
- impulsivity;
- working-memory difficulties;
- time blindness;
- difficulty switching attention;
- executive dysfunction;
- difficulty initiating tasks;
- reduced motivation for delayed rewards.
A child with a PDA profile may resist because the request itself creates pressure or a perceived loss of autonomy.
Some children are both autistic and have ADHD. Their behaviour may therefore arise from several interacting needs rather than one single cause.
A thorough assessment should explore the child’s whole presentation instead of assuming every refusal has the same explanation.
PDA and anxiety
Anxiety is frequently associated with severe demand avoidance, but it may not look like visible worry.
In children, anxiety can appear as:
- anger;
- silliness;
- controlling behaviour;
- repeated negotiation;
- avoidance;
- perfectionism;
- physical complaints;
- shutdown;
- aggression;
- apparent indifference.
Asking “Are you anxious?” may not produce a useful answer.
The child may:
- not recognise the feeling;
- be unable to describe it;
- fear admitting it;
- experience the question itself as another demand.
Adults may gain more information by observing patterns, identifying triggers and discussing experiences once the child feels safe and regulated.
How is a PDA profile assessed?
Because PDA is not a standalone diagnosis, a child suspected of having a PDA profile would usually be considered through a broader autism assessment.
A comprehensive assessment may consider:
- developmental history;
- information from parents or carers;
- information from school;
- communication and social interaction;
- sensory processing;
- emotional regulation;
- anxiety;
- executive functioning;
- behaviour across different environments;
- alternative or co-occurring conditions.
Assessment should not depend entirely on how the child behaves during one appointment.
A child may mask, comply temporarily or engage well with an unfamiliar professional in a calm one-to-one environment. This does not necessarily reflect how they function at home, school or in busy community settings.
Developmental history and evidence from several environments are therefore particularly important.
Parents considering assessment can explore the School of Diversity information about private ADHD and ASD assessments.
Can a child show PDA traits without an autism diagnosis?
A child may show severe demand avoidance before receiving an autism diagnosis.
Some children and adults may also identify strongly with descriptions of PDA without having completed a formal assessment.
However, PDA is most commonly understood as an autism-related profile. Assessment should consider the person’s full developmental presentation rather than attempting to identify PDA in isolation.
Other possible contributors to demand avoidance can include:
- anxiety;
- ADHD;
- sensory processing differences;
- communication difficulties;
- learning needs;
- trauma;
- depression;
- obsessive-compulsive difficulties;
- school-related distress;
- sleep problems;
- physical pain or illness.
The purpose of assessment should not simply be to find the correct label. It should explain the person’s needs and identify support that is likely to help.
Supporting a child with a PDA profile at home
There is no universal strategy.
What reduces pressure for one child may create uncertainty for another. Support should therefore be individualised, respectful and focused on emotional safety and regulation.
Reduce unnecessary demands
Consider which expectations are essential and which can be:
- delayed;
- adjusted;
- combined;
- offered as a choice;
- temporarily removed.
Reducing demands does not mean abandoning all routines or boundaries.
It means recognising that a highly dysregulated child cannot learn effectively through escalating pressure.
Prioritise safety and connection
During severe distress, the immediate priorities are:
- reducing threat;
- keeping everyone safe;
- using less language;
- avoiding arguments;
- allowing time for recovery.
Reasoning, consequences and problem-solving are more effective after the child has become regulated.
Use collaborative language
Direct commands can increase the child’s perception that control is being removed.
Collaborative alternatives may include:
- “I wonder how we could do this.”
- “Would it help to start together?”
- “Which part feels manageable?”
- “We have two possibilities.”
- “Let’s see whether there is another way.”
- “I’m going to leave this here.”
- “Could we make a plan that works for both of us?”
The purpose is not to disguise demands through clever wording.
Children often recognise artificial choices or indirect manipulation. Communication should remain honest and respectful.
Offer meaningful choices
Choices can restore a sense of control.
For example:
- now or in ten minutes;
- upstairs or downstairs;
- written work or spoken response;
- shoes first or coat first;
- complete one section or use an alternative activity;
- work alone or begin with an adult.
Avoid presenting a false choice when only one response will actually be accepted.
Use declarative language
Declarative language shares information without immediately requiring the child to act.
Instead of:
“Put your coat on now.”
Try:
“It looks cold outside.”
Instead of:
“Come and eat your dinner.”
Try:
“Dinner is on the table when you’re ready.”
Instead of:
“Start your homework.”
Try:
“I can see the worksheet is still in the bag.”
This approach will not work in every situation, but it can reduce the feeling of being directed.
Build in recovery time
School, appointments, visitors and social activities may require significant masking and regulation.
A child may need:
- quiet time;
- reduced conversation;
- access to a preferred activity;
- lower lighting;
- comfortable clothing;
- food available without pressure;
- freedom from questions after school;
- time alone without being expected to explain themselves.
Recovery should be treated as a legitimate need, not a reward that must be earned.
Prepare without overwhelming
Predictability can reduce anxiety, but too much advance notice can sometimes allow anxiety to build.
Some children require detailed preparation. Others manage better with short notice and flexible plans.
Parents may need to experiment with:
- visual information;
- written choices;
- brief reminders;
- flexible time windows;
- avoiding repeated countdowns;
- sharing only the information the child needs.
Use humour carefully
Humour, novelty and playfulness may reduce the intensity of a request.
However, humour should never:
- mock the child;
- minimise their distress;
- turn anxiety into entertainment;
- be used to trick the child into complying.
Avoid power struggles
Once an interaction becomes a contest over who is in control, both the demand and the relationship can become more threatening.
Where possible:
- pause;
- reduce language;
- reconsider the immediate objective;
- return to the issue later;
- try a different method;
- focus on the underlying barrier.
Review rewards and consequences
Rewards, sanctions and behaviour charts often assume that the child can comply consistently when sufficiently motivated.
For a child whose nervous system is reacting to pressure, increasing the reward or punishment may simply increase the demand.
Adults should ask:
- Does the child understand the task?
- Can they begin it?
- Are they regulated enough to respond?
- Is the environment contributing to the difficulty?
- Does the reward create additional expectation?
- Is the consequence increasing anxiety?
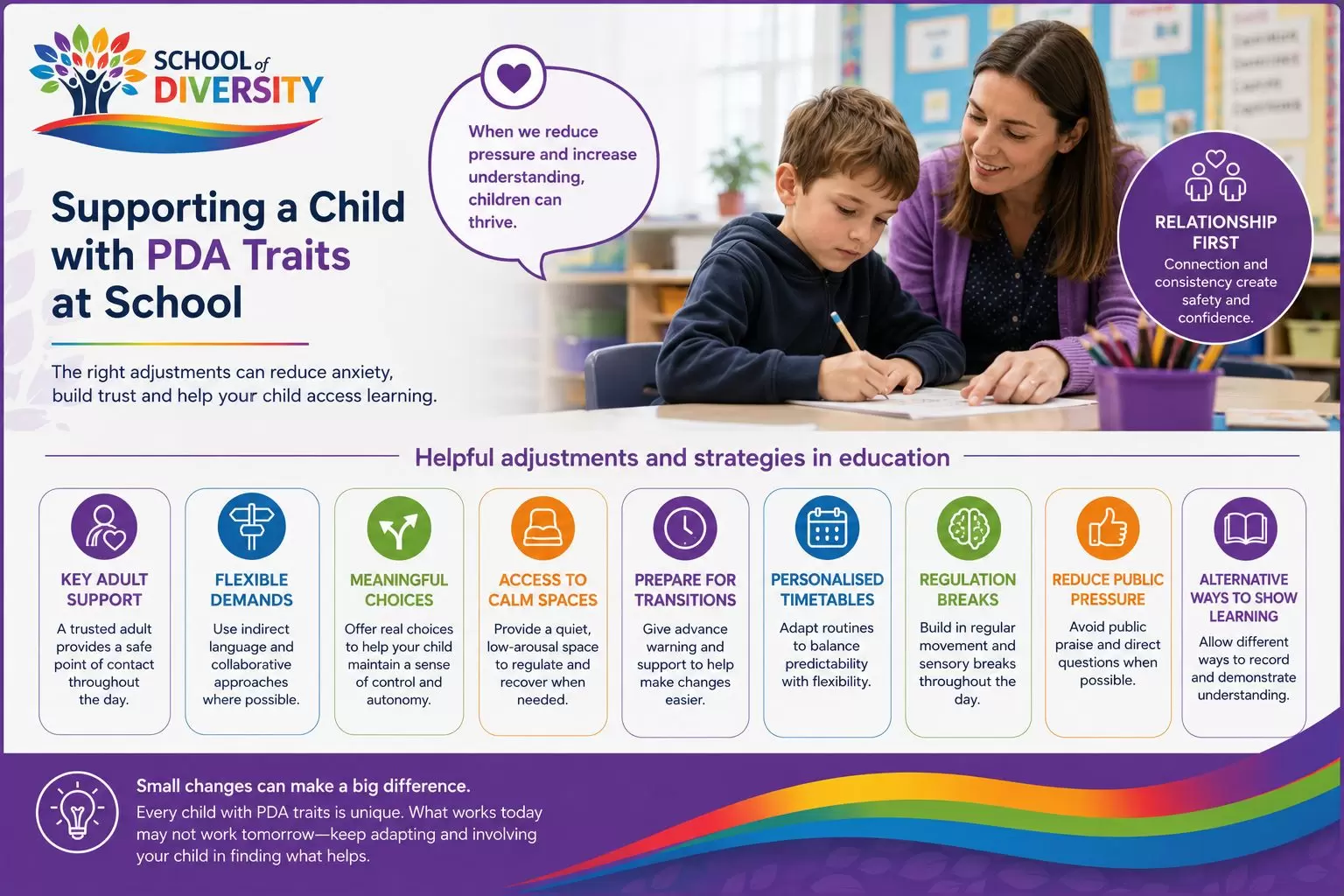
Supporting a child with PDA traits at school
A child with severe demand avoidance may require an individualised approach rather than a standard behaviour-management programme.
Helpful adjustments may include:
- a trusted key adult;
- flexible arrival arrangements;
- reduced direct questioning;
- choices about how work is completed;
- access to a low-arousal space;
- permission to take regulation breaks;
- alternative methods of recording work;
- reduced public praise;
- preparation for transitions;
- flexibility around uniform or sensory demands;
- a personalised timetable;
- lower-demand communication;
- support during unstructured periods;
- planned recovery after demanding activities;
- staff training in autism, anxiety and demand avoidance;
- a written regulation and distress plan.
Strategies should be applied consistently.
A child may become more anxious if one adult uses a flexible, collaborative approach while another insists on rigid compliance.
Parents who need practical help preparing for school discussions can explore our collection of parent SEN resources and support.
PDA, school avoidance and attendance difficulties
For some children, school becomes associated with continual demand.
These demands can include:
- getting ready at a fixed time;
- wearing a uniform;
- travelling;
- entering a busy building;
- following instructions;
- changing lessons;
- completing work;
- responding socially;
- tolerating noise;
- eating at set times;
- remaining in one place;
- coping with uncertainty.
Over time, school attendance itself may begin to trigger a threat response.
This can result in:
- lateness;
- difficulty leaving home;
- distress at the school entrance;
- running away;
- physical symptoms;
- Sunday-evening anxiety;
- exhaustion;
- increasing absence;
- inability to return after holidays.
The child should not automatically be treated as choosing non-attendance.
Parents and schools should investigate:
- unmet special educational needs;
- sensory stress;
- bullying;
- academic pressure;
- social demands;
- fear of failure;
- unpredictable routines;
- disciplinary approaches;
- insufficient recovery time.
Attendance plans that increase pressure without addressing the causes of distress may make the situation worse.
Can PDA-related needs be included in an EHCP?
Yes.
An Education, Health and Care Plan should describe a child’s special educational needs and specify the provision required to meet them.
The provision should be based on the child’s functional needs. A separate PDA diagnosis is not required.
Relevant needs might include:
- extreme anxiety in response to demands;
- difficulty initiating and completing tasks;
- sensory sensitivities;
- emotional dysregulation;
- difficulty accessing a conventional classroom;
- distress during transitions;
- masking followed by exhaustion or meltdowns;
- difficulty tolerating direct instruction;
- school-attendance difficulties;
- reduced communication when overwhelmed.
Parents who are new to the process can begin with our guide explaining what an EHCP is and how it works.
Where a child’s needs cannot reasonably be met through ordinary SEN Support, parents may need to consider how to apply for an EHCP.
For autistic children specifically, our EHCP for autism guide explains the types of needs and provision that may need to be recorded.
What should an EHCP say about demand avoidance?
An EHCP should not merely state that the child “dislikes demands” or “can be oppositional.”
Section B should describe the child’s needs accurately and neutrally.
This may include:
- anxiety triggered by direct demands;
- reduced ability to initiate tasks under pressure;
- difficulty tolerating uncertainty;
- sensory factors contributing to distress;
- masking within structured environments;
- inability to communicate effectively when dysregulated;
- a strong need for predictability and autonomy;
- the impact on attendance and access to learning.
Section F should then specify the provision required to meet each identified need.
Depending on the evidence, this may include:
- a named or consistently available key adult;
- staff trained in autism and demand avoidance;
- a low-arousal communication approach;
- reduced use of direct commands;
- meaningful choices within learning activities;
- flexible methods of recording work;
- access to a quiet regulation space;
- planned sensory and emotional-regulation breaks;
- individual transition support;
- a personalised attendance plan;
- occupational therapy input;
- speech and language therapy;
- psychological advice;
- regular monitoring and review.
Provision should explain:
- who will provide it;
- how often it will be provided;
- how long sessions or support will last;
- what training staff require;
- how progress will be reviewed;
- what happens when the child becomes distressed.
Vague wording such as “access to support,” “regular opportunities for breaks” or “staff will use appropriate strategies” may be difficult to monitor and enforce.
What evidence should parents collect?
A clear evidence record can help schools, assessors and local authorities understand that the child’s behaviour is patterned and need-led.
Parents may record:
- the demand or expectation;
- the child’s initial response;
- signs of anxiety or dysregulation;
- avoidance strategies used;
- what adults did next;
- whether pressure increased or decreased;
- what helped;
- how long recovery took;
- differences between home and school;
- effects on sleep, eating or toileting;
- the child’s own explanation where available.
It is also helpful to document cumulative demand.
The final incident of the day may not be the true cause of the distress. A child may have coped with dozens of demands before one apparently small request becomes unmanageable.
Evidence can include:
- parent diaries;
- emails to school;
- attendance records;
- behaviour logs;
- photographs where appropriate;
- SEN Support plans;
- meeting notes;
- school reports;
- professional assessments;
- examples of work not completed because of distress;
- records of successful adjustments.
Our guide to EHCP evidence for parents explains how parent, school and professional evidence can be organised.
Questions to ask the school or assessor
Parents may find the following questions helpful:
- What do you believe is driving the demand avoidance?
- Have autism, ADHD, anxiety and sensory needs been considered?
- Could my child be masking at school?
- How are my child’s views being gathered?
- What happens when pressure is reduced?
- Does my child respond differently to collaborative language?
- Are staff interpreting distress as deliberate defiance?
- What reasonable adjustments have been tried?
- Have the adjustments been used consistently?
- What support is available before my child reaches crisis?
- Does my child require SEN Support or an EHC needs assessment?
- Can the assessment describe the demand-avoidant profile even if the term PDA is not used?
- What training do the adults supporting my child require?
Questions should focus on understanding the child rather than proving who is right.
What not to assume about a child with PDA traits
A child who avoids demands is not necessarily:
- lazy;
- deliberately manipulative;
- badly parented;
- choosing to fail;
- attention seeking;
- lacking boundaries;
- unwilling to learn;
- unaffected because they behave well at school.
Behaviour communicates that something is happening, but adults must investigate carefully before deciding what it means.
The same outward behaviour can arise from different causes. Effective support depends on identifying the cause rather than responding only to what adults can see.
When should families seek professional support?
Professional advice may be appropriate where demand avoidance is significantly affecting:
- education;
- school attendance;
- family relationships;
- personal care;
- sleep;
- eating or drinking;
- toileting;
- emotional wellbeing;
- safety;
- access to the community.
Parents do not need to wait until their child reaches crisis.
Support may come from:
- the school SENCO;
- a GP;
- a paediatrician;
- an educational psychologist;
- a clinical or counselling psychologist;
- a speech and language therapist;
- an occupational therapist;
- an autism assessment service;
- a SEND adviser or advocate.
Families who need broader practical guidance can also use the Parent Power Pack, which includes resources on reasonable adjustments, regulation, evidence gathering, school communication and emotionally based school avoidance.
Urgent professional support should be sought where there is:
- immediate risk of serious harm;
- severe restriction of food or fluids;
- significant self-injury;
- suicidal thoughts;
- an acute mental-health crisis.
Frequently asked questions about PDA autism
Is PDA an official diagnosis in the UK?
No. PDA is not currently a standalone clinical diagnosis. Some professionals may describe an autistic person as having a PDA or demand-avoidant profile.
Does every autistic child avoid demands?
Many autistic children avoid certain demands because of anxiety, sensory discomfort, communication needs or executive-function difficulties. This does not necessarily mean they have a PDA profile.
Can a child with PDA behave well at school?
Yes. Some children mask or comply at school and release accumulated distress at home.
School behaviour must therefore be considered alongside parent evidence, attendance patterns, exhaustion and the child’s wider wellbeing.
Are children with PDA deliberately controlling?
Control may be a way of creating safety, reducing uncertainty and protecting autonomy.
The behaviour can still be difficult for families and schools, but understanding its function usually leads to more effective support than blame or punishment.
Do reward charts work for PDA?
Some children may tolerate reward charts, but others experience them as an additional demand.
Where a chart increases anxiety, adults should focus on understanding barriers, reducing threat and developing a collaborative approach.
Can PDA affect enjoyable activities?
Yes.
Once an enjoyable activity becomes expected, scheduled, observed or repeatedly discussed, it may begin to feel like a demand.
Can adults have a PDA profile?
Yes. Demand avoidance and a strong need for autonomy may continue into adulthood.
Adults may develop sophisticated ways of masking, delaying, negotiating or structuring their lives to minimise external demands.
Can PDA be mentioned in an autism assessment report?
Potentially.
Some clinicians record a PDA or demand-avoidant profile. Others describe the relevant characteristics, anxiety and support recommendations without using the PDA label.
Does my child need a PDA diagnosis to receive school support?
No.
School support should be based on the child’s identified needs. A child does not need a separate PDA diagnosis before reasonable adjustments, SEN Support or EHCP provision can be considered.
Can a child receive an EHCP without an autism or PDA diagnosis?
Yes.
EHCP decisions are based on the child’s special educational needs and the provision they may require, not solely on diagnostic labels.
Final Thoughts
Severe demand avoidance should not be reduced to a battle over behaviour.
For some autistic children, everyday expectations can trigger a powerful response involving anxiety, uncertainty, loss of control and nervous-system threat.
The most effective support begins with curiosity.
- What is the child finding difficult?
- What pressure can be reduced?
- What sensory or communication needs are being missed?
- How can the child retain meaningful autonomy?
- What adjustments would make the environment feel safer?
- What evidence is needed to secure consistent support?
When parents, schools and professionals move away from blame and towards understanding, children are more likely to feel safe, remain connected and gradually develop ways to manage demands without becoming overwhelmed.
For more guidance, explore our resources and support for parents of neurodivergent children or learn more about SEN support, autism and neurodiversity.
This article provides general information and should not replace an individual clinical, educational or legal assessment.